The number of babies born with severe congenital heart defects will increase because of new U.S. abortion bans, potentially straining the health care system’s capacity to meet their needs, according to research from the Stanford School of Medicine.
The study, which published Aug. 3 in Obstetrics and Gynecology, focused on a group of congenital heart conditions known as single-ventricle cardiac defects. Even with the best medical and surgical care, these
conditions are fatal for 10% to 30% of affected infants.
The heart defects are usually diagnosed at a prenatal ultrasound around 20 weeks of pregnancy,
prompting some parents to opt for an abortion. However, when the 2022 U.S. Supreme Court decision
Dobbs v. Jackson Women’s Health Organization removed federal constitutional protections for abortion,
it became unavailable in many U.S. states, with uncertain consequences for the health care system.
“We wanted to understand how abortion bans are going to impact hospital resources for newborns born
with cardiac anomalies,” said the study’s lead author, Hayley Miller, MD, a fellow in maternal-fetal
medicine. “Our analysis of the impact on health systems can help inform legislators of the realities of
medical care with abortion restrictions. Some states will have incredibly impacted neonatal and cardiac
intensive care units.”
The study’s senior author is Yair Blumenfeld, MD, professor of obstetrics and gynecology. The research
team includes Stanford Medicine experts in maternal-fetal medicine, complex family planning and
pediatric cardiology.
When more infants are born with severe heart defects, some hospitals may not have the resources to
provide the intensive care services and open-heart surgeries that are needed. The resulting demand for
neonatal intensive care unit beds could also affect newborns with other medical problems. Similarly, the
demand for cardiac resources — including cardiac ICU beds — may be limited for other children with
heart disease.
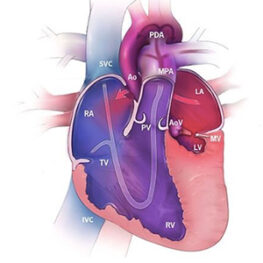
Missing heart chamber
The heart normally has four chambers: two atria, and two ventricles, which are larger and are the heart’s
main pumps. The right ventricle pumps blood through the lungs to pick up oxygen. The left ventricle
pumps oxygenated blood to the rest of the body.
Hypoplastic left heart syndrome, one of the most common forms of single-ventricle cardiac defect, is a
devastating diagnosis for expectant parents to receive midway through pregnancy. It occurs when the left
ventricle does not form correctly before birth. The syndrome also includes malformation of valves that
normally maintain one-way blood flow through the heart, and of the aorta, the large blood vessel that
carries blood away from the heart to the rest of the body. Without treatment, this heart defect is always
fatal in infancy.
The condition can be treated with three open-heart surgeries performed in the first two to three years of
life. The surgeries reroute blood so that the right ventricle pumps oxygen-rich blood throughout the body
instead of pumping only to the lungs. Although the surgeries can be lifesaving, they do not restore normal heart structure. Even with excellent surgical care, some patients die in infancy or childhood, and others suffer damage to the brain, lungs, liver, kidneys or intestines. Some affected children receive a heart transplant instead, which provides a heart with normal physiology but also requires a lifetime of immune- suppressing drugs to prevent rejection of the organ.
“Because of the guarded prognosis and difficult life that faces children born with single-ventricle diseases, termination of pregnancy is offered at most major hospitals following diagnosis,” said Shiraz Maskatia, MD, a fetal cardiologist at Stanford Medicine and a co-author on the study. “A universal, 20-week ban on abortion limits treatment options for doctors and families and creates a heavier demand for other health care resources.”
In the study, the authors used mathematical models to estimate how many more infants with single-
ventricle cardiac defects would be born each year under three different abortion-ban scenarios, as
compared with the rate of these births before the 2022 Dobbs decision. Before 2022, abortion was legal
across the country until approximately 24 weeks of pregnancy. The scenarios the researchers used for
modeling were national bans on abortion after 20 weeks’ gestation, 13 weeks’ gestation and a complete
abortion ban at any stage of pregnancy. Abortion policies now vary from state to state and are still in flux, so the researchers modeled what would happen under national scenarios for simplicity’s sake.
The study’s models predicted that under pre-Dobbs laws, about 1,006 infants would be born each year
with single-ventricle cardiac defects, which is similar to the U.S. Centers for Disease Control estimate of
1,025 cases per year. The model predicted that, in their first year, these babies would need 986 heart
surgeries, 28 heart transplants and 142 uses of extracorporeal membrane oxygenation support. ECMO
provides mechanical support like that of a heart-lung machine and is used for some infants awaiting heart surgery if medication does not stabilize them. The researchers studied ECMO use because it is complex and high risk, requiring a highly trained care team and specialized equipment. The model also predicted 189 newborn deaths per year from single-ventricle cardiac defects.
If a complete abortion ban were enacted nationwide, the models predicted that 1,547 babies born each
year would be affected by single-ventricle cardiac defects, an increase of 541 affected newborns per year.
This would result in 1,517 heart surgeries, 44 heart transplants, 219 ECMO utilizations and 291 neonatal
deaths. Modeling the outcomes for national abortion bans at 13 and 20 weeks of gestation led to
intermediate predictions for all outcomes, with more affected births, heart surgeries, ECMO utilizations
and deaths than under pre-Dobbs laws but fewer than under a complete abortion ban.
A ban at or before 20 weeks of pregnancy prevents a family from choosing an abortion after diagnosis of a severe heart condition, as defects cannot reliably be diagnosed earlier, Miller said. She added that the
researchers do not aim to promote abortions for these pregnancies but recognize that families may
choose abortion for personal reasons. “Some families want to avoid the trauma that accompanies
neonatal death, or they realize that having a newborn who will require major surgeries and prolonged
NICU stays in the first year of life might change family dynamics in a way they cannot support,” she said.
“The research team hopes that legislators passing abortion restrictions will thoroughly consider the
effects of these laws on patients, families, hospitals and health care systems,” Miller said.
“Not only will the need for NICU beds be increased, but more ECMO machines and heart transplants,
which are already in short supply, will be needed for babies born in states with restrictive bans,” she said.
“Based on my understanding from colleagues in restrictive states, they are now seeing dramatic increases in need for hospital resources, and seeing newborns who must be hospitalized far away from home to get a NICU bed.”
The Dunlevie Maternal-Fetal Medicine Center for Discovery, Innovation and Clinical Impact at Stanford
University provided funding for the study.